Why Testosterone Levels are Falling in Young Men, & How We Can Restore Them


During my first two years of college, I struggled with low testosterone and several of its consequences, including erectile dysfunction, high blood pressure, and low self esteem.
How could this be? At the ripe young age of 18-20, my testosterone levels should have been at their peak, especially given that I was well muscled and trained as a college football player. But I'm not alone...
The Reddit post below is just one of many of young men reporting their struggles with low testosterone.
My experience and that of thousands of other men is validated by recent scientific research which discovered a significant decline in the testosterone levels of men aged 15-39 years old (12). More on that later...
This begs the question: why are so many men, many of whom are young and active, struggling with low testosterone?
This question has been the core driver of my life's work: to reverse trends in declining male reproductive health.
Over the past five years, I have overcome low testosterone, published an award-winning thesis on male reproductive health, and founded a men’s health coaching business alongside my career as a certified personal trainer.
My Transformation: From Sub-Par to Optimal Testosterone


A picture speaks a thousand words. This is my four year transformation from sub-par to optimal testosterone levels. On the left is me at age 19, on the right is me at age 23.
So if you're one of the many thousands of men struggling with low testosterone, read on...
In this article, I’m going to break down why testosterone levels are falling, and what you can do about it, by providing actionable, evidence-based protocols that you can directly apply to your life to optimize your testosterone levels naturally.
Without further adieu, let's dive into the research.
Study Breakdown: "Decline in Testosterone Levels Among Adolescent and Young Adult Men in the USA"
A 2021 study found a significant decline in the testosterone levels of men aged 15-39 (12), termed "adolescent and young adult males,” abbreviated as “AYA males.”
At the time of publication, the researchers reported that 1 in 5 AYA men had testosterone deficiency.
While past research established testosterone decline in men of all ages (19), this was the first study to document the trend in AYA men specifically.
The team analyzed data from the National Health and Nutrition Examination Surveys (NHANES), which measured testosterone levels in 4,055 men between 1999–2016, across five survey cycles.
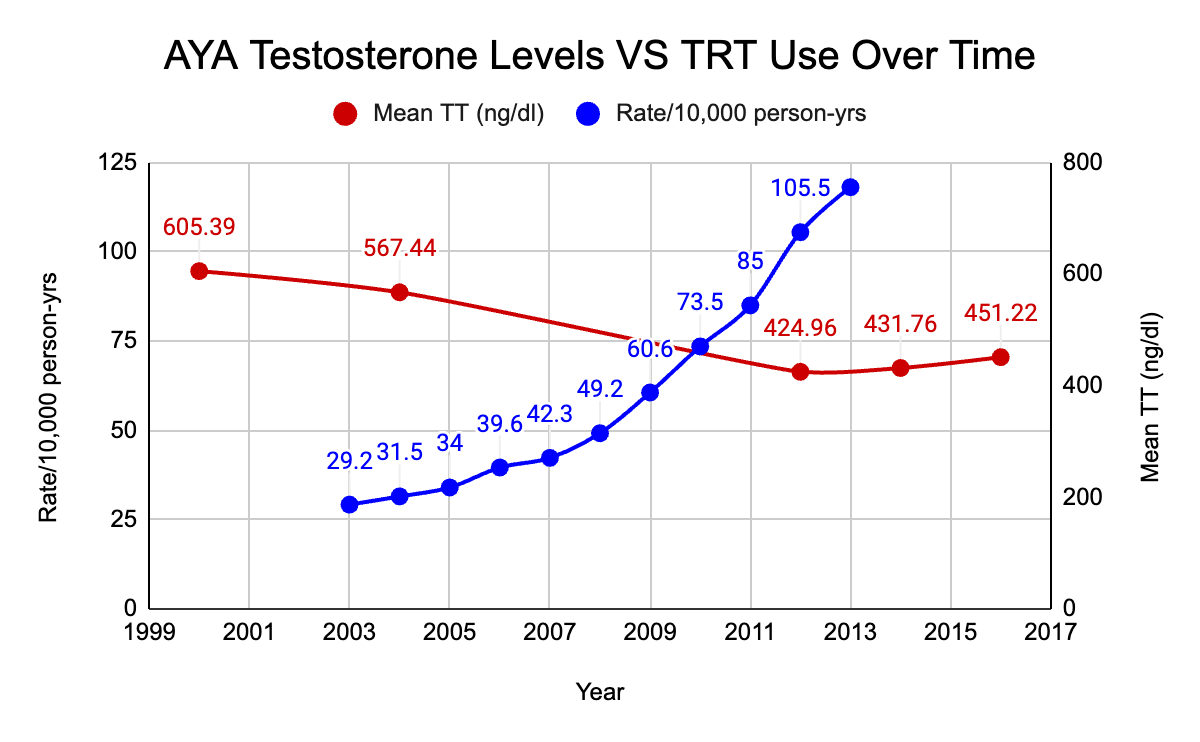
I’ve visualized their reported averages in the line graph below.
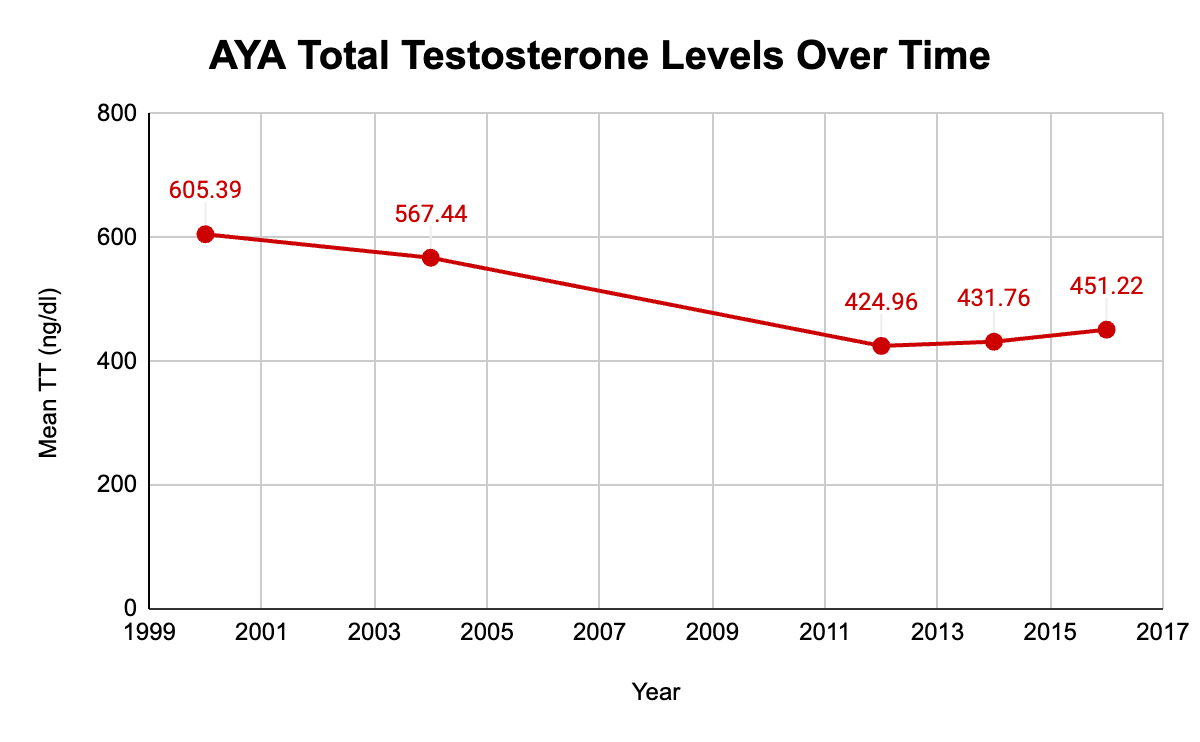
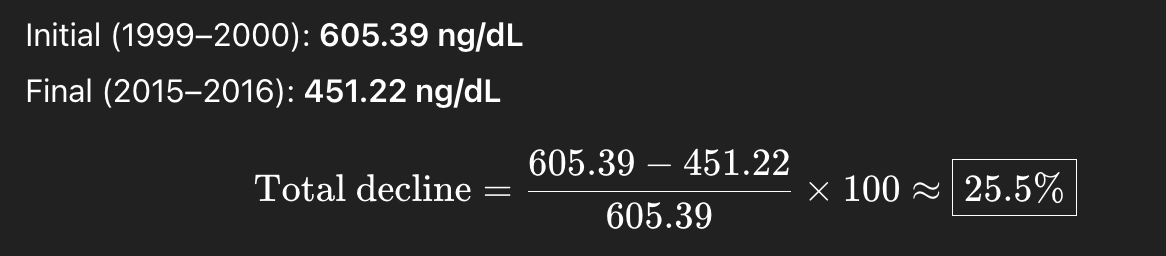
The researchers found that average testosterone fell from 605.39 ng/dL in 1999–2000 to 451.22 ng/dL in 2016 (p < 0.001), a 25.5% decrease.
This works out to an average decline of about 1.59% per year.

The Future of Testosterone: Will Low T be the Norm?
If testosterone levels continued to fall at that rate, the population average would reach the clinical threshold for low testosterone (300 ng/dL) by 2026.
Translation: assuming these trends continue, low testosterone will be the new normal.

To be clear: this thought experiment is a projection, not a prophecy. Statistical extrapolation is simply predictive based on known data.
Just because testosterone levels have declined at this rate in the past doesn't guarantee that they will in the future. They may rebound, continue to decline, or plateau, largely depending on whether or not we make changes for the betterment of men’s health.
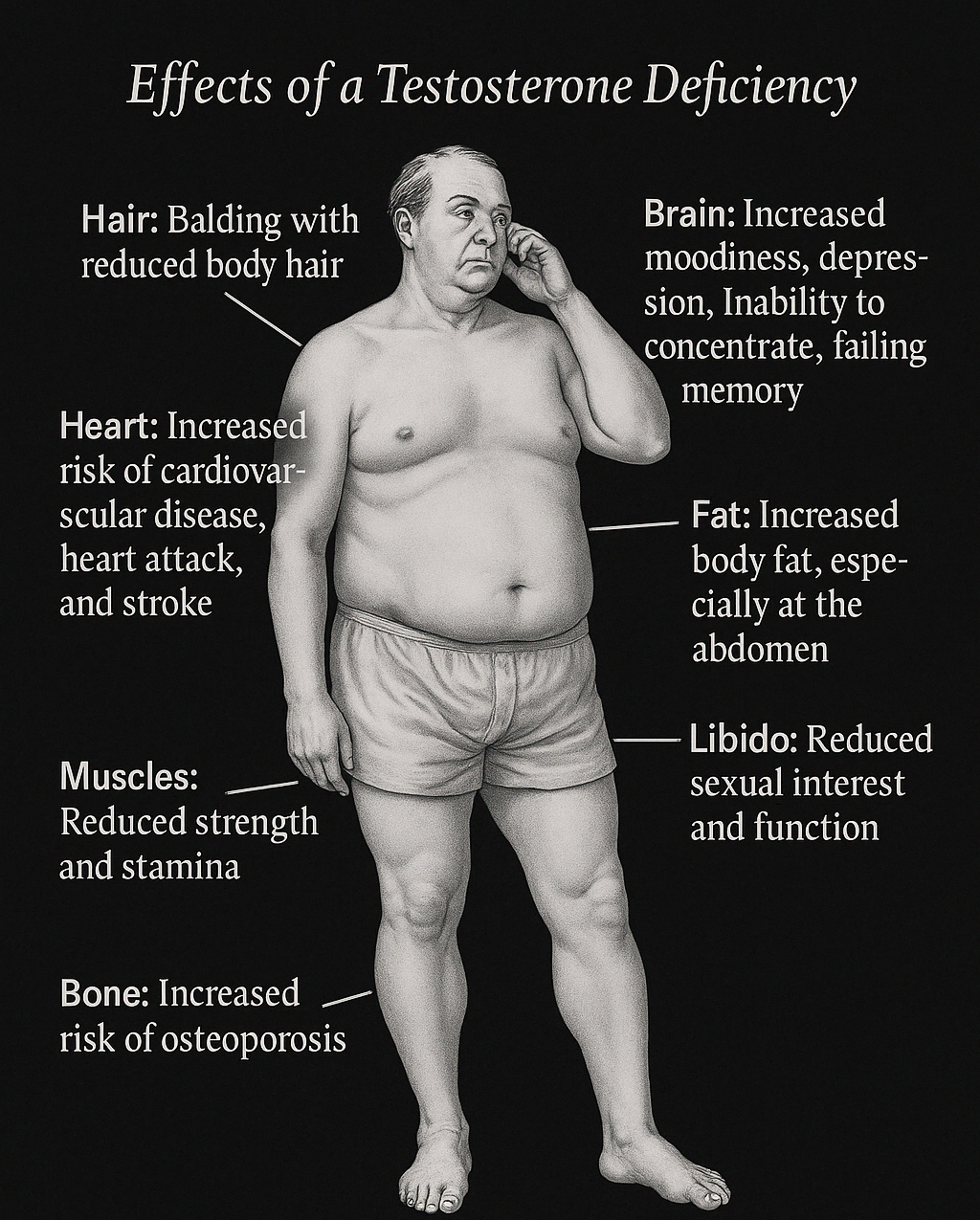
What Low T Feels Like (Sound Familiar?)
Since numerical measures of subjective experience can be difficult to conceptualize, I've described common symptoms of low testosterone to help you viscerally understand the consequences of these statistics for the wellbeing of men in society.
1. Cognitive & Mood Changes
- Brain fog: Slower thinking, forgetfulness, lack of clarity
- Low motivation: Things that once excited you now feel like chores
- Mood instability: More irritable, reactive, or depressive without clear reason
- Reduced stress resilience: Less confident, more anxious under pressure
- Loss of edge: Diminished assertiveness, drive, and competitiveness
2. Physical Energy & Strength
- Fatigue: Morning energy fades fast; you rely more on caffeine and naps
- Slower recovery: From workouts, injuries, even stressful days
- Loss of strength: Especially in compound lifts; plateaus come sooner, gains fade faster
- Decreased muscle tone: Softer, less defined physique even if weight remains stable
3. Body Composition
- Increased body fat: Calories seem to be stored as fat more easily
- Gynecomastia risk: Slight breast tissue growth or puffier nipples
- Harder to gain muscle: Lifting in the gym doesn't elicit gains well
- Insulin resistance: Blood sugar regulation becomes less efficient
4. Sex Drive & Performance
- Decreased libido: Less spontaneous arousal, more need for mental stimulation or novelty
- Weaker erections: Less frequent morning wood, weaker rigidity
- Reduced ejaculation volume & intensity
- Longer recovery time: Between sexual encounters or arousals
As you can see, low testosterone causes pain in all domains of a man's life, so it's no surprise that men are turning to Testosterone Replacement Therapy (TRT) at an unprecedented rate...
The Rise of TRT Use In Young Men

A 2016 study found that the rate of Testosterone Replacement Therapy (TRT) use among 18 to 45-year-old men quadrupled between 2003-2013 (16).
This was more than the threefold increase seen in older men (56 to 64 years old).
Overlaying the trends in testosterone levels and TRT use over time reveals inverse correlation between them: as testosterone levels have fallen, TRT use has risen.
TRT is an attractive solution because it promises immediate relief with little effort.
However, nothing worth having, including healthy testosterone levels, comes without effort.
The cost of the near instant, effortless relief provided by TRT is paid for by its long term-consequences, which most men are completely unaware of...
#1 Side Effect of TRT Every Man Should Know
Of all the undesirable side effects of TRT, there’s one that is especially concerning for young men.
It is well established in the scientific literature that TRT is a contraceptive, meaning it can cause infertility (14). Here's how...
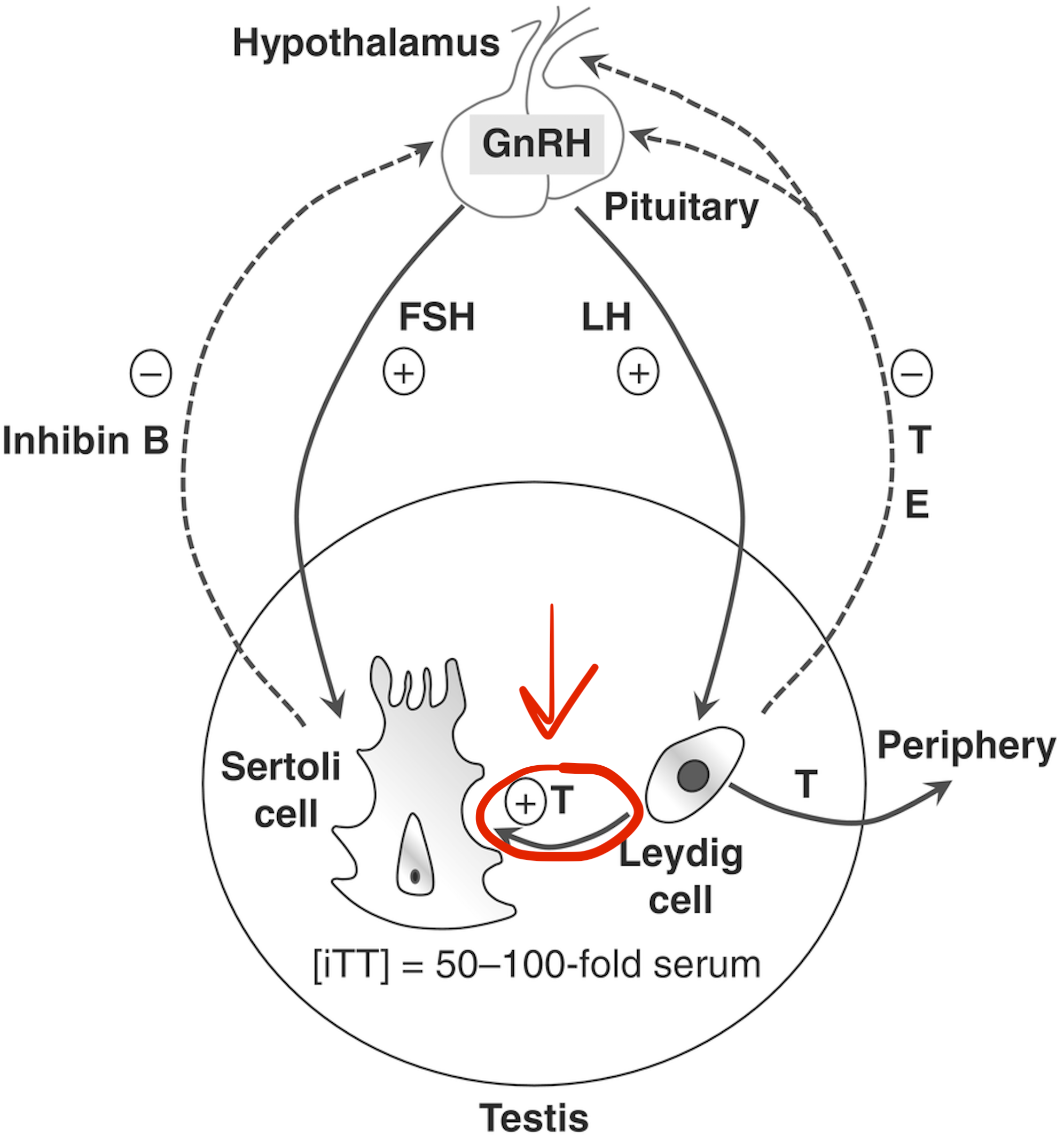
Testosterone & Sperm Production
Testosterone is a key driver of spermatogenesis (the process of sperm production), which is required for a man to reproduce.
Both testosterone and sperm are produced inside the testes (in Leydig and Sertoli cells respectively).
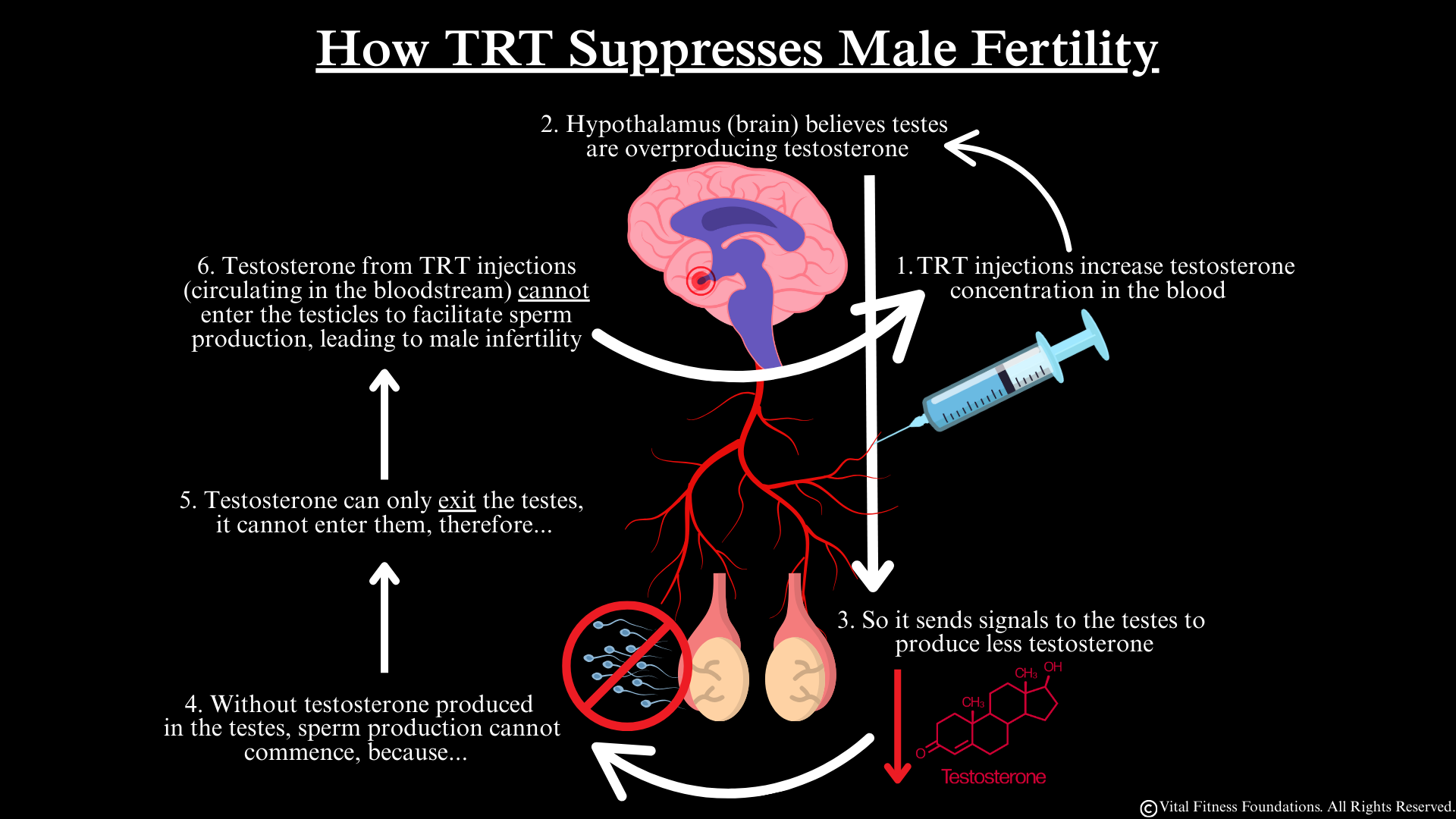
TRT Causes Male Infertility
When exogenous (external) testosterone (such as TRT or anabolic steroids) is introduced into the bloodstream, the body detects this surplus and responds by downregulating endogenous (internal) testosterone production in the testes to keep levels in proper balance (termed homeostasis).
Simply put, TRT deceives the body into believing it has plenty of testosterone, causing it to stop producing its own.
The problem is that only endogenous testosterone is capable of stimulating sperm production, not exogenous testosterone like TRT.
This is because testosterone can only exit the testes, so exogenous testosterone in the bloodstream cannot enter them to facilitate sperm production.
Therefore, only endogenous testosterone naturally produced within the testes can promote sperm production.
Since TRT causes the body to stop producing endogenous testosterone, and cannot facilitate sperm production itself, TRT use leads to the cessation of sperm production, and as a result, male infertility.
Can Fertility be Recovered After TRT use?
Although clinical trials report that TRT induced infertility is reversible in most cases, recovery of fertility can take up to two years (14).
These clinical trials were carefully monitored and used conservative doses of TRT over a limited time duration, all of which favor a best case scenario for fertility recovery. The researchers explicitly mentioned that in actual practice, recovery may not be as likely (14).
What Your Doctor Might Not Know About TRT
A 2012 survey found that 25% urologists (doctors who specialize in male reproductive health), reported that they would treat infertile males with TRT (9), which, as we've established, is paradoxical because TRT suppresses male fertility.
Given the ignorance regarding the side effects of TRT among urologists, one can only wonder to what degree primary care providers, who are generalists, m unaware of its effects.
Lack of awareness of the side effects of TRT among medical practitioners could lead to unnecessary prescription and mismanaged treatment, with the burden of unintended consequences unknowingly carried by the men who use it.
TRT Doesn't Address Root Cause
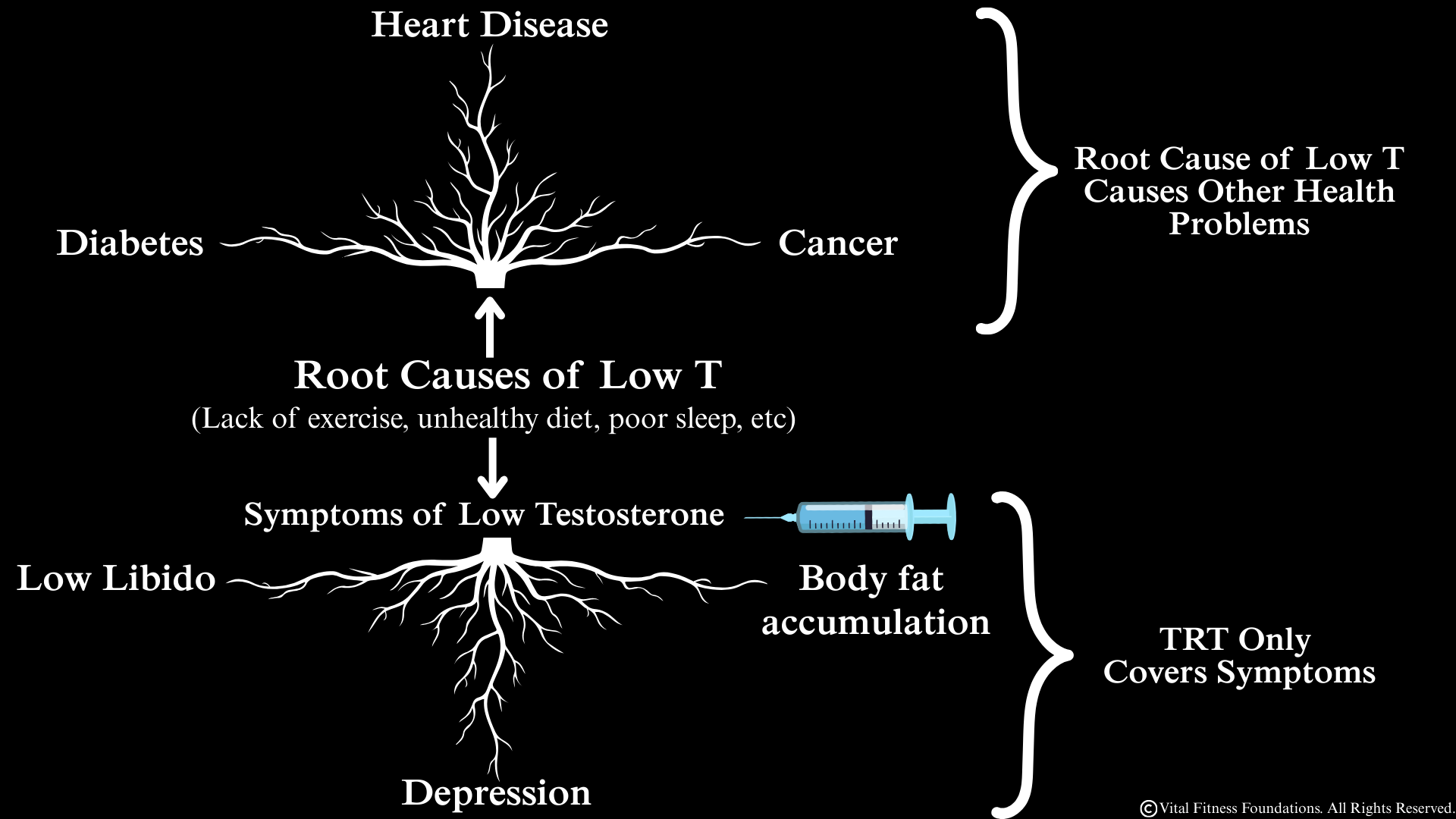
The other problem with TRT is it merely masks the symptoms of low testosterone without addressing its root causes.
This is dangerous, because the body functions as an interconnected system, so the underlying factors that cause low testosterone will continue to persist even after TRT treats the symptoms.
For example, lack of exercise is a common contributing factor to low testosterone, as well as most other chronic diseases.
If a non-exercising man with low testosterone were treated with TRT, he may continue to go on living without exercising, because the treatment relieved symptoms, giving him no incentive to address the root cause; insufficient exercise.
As a result, he may develop other health conditions consequent to a lack of exercise, like heart disease, diabetes, cancer, etc.
Since young men have more life ahead of them than older men, unaddressed root causes of low testosterone have many more years to contribute to the development of other chronic diseases.
The problems with TRT aside, the central issue remains; men wouldn't feel compelled to use TRT if they didn't have low testosterone in the first place.
So instead of vilifying TRT, our focus should be on what's in one's control: their lifestyle choices.
Gaps Between Science & Reality
Aside from genetic hypogonadism, most of the causes of low testosterone can be remediated through changes in lifestyle, which is why TRT is almost always unnecessary.
To make those lifestyle changes as practical as possible, I’m going to summarize the causes of testosterone decline the researchers hypothesized in the study (12).
But before I do, there are three main limitations of this research that you should be aware of.
- The researchers hypothesized potential causes of low testosterone without suggesting any solutions to reverse them.
To make up for this, I'm going to supplement the research by providing a solution for each cause of low testosterone in a "causes and solutions" sequence.
- The researchers didn’t include all the potential causes of low testosterone worth considering.
Since their primary goal was to track testosterone levels over time, it would be out of the scope of their study to systematically review all of the potential causes of low testosterone.
To account for this, I’m going to expand upon their list using other studies as well as my own experience.
- In science there is often a disconnect between theories and reality.
Imagine a group of researchers in lab coats discussing the reasons why testosterone levels might be declining in AYA men.
Although researchers are well-informed experts, their ideas entirely come from academic papers and textbooks, not from directly engaging with men living with low testosterone.
This dynamic is analogous to the relationship between generals and soldiers in war.
Generals are usually too preoccupied with devising battle plans to get a feel for the morale of the troops.
Likewise, the perspective of the researchers is limited due to the gap between their conceptual book knowledge and the reality of life for men suffering from low testosterone; a gap which my boots on the ground experience perfectly fills….
Not only have I overcome low testosterone in my own life, but as a seasoned men’s health coach and personal trainer, helping “the troops” is literally my job.
My experience extends back to my recent college years where I played football with over 150 teammates; all young men who fit the demographic studied in the research.
As such, I have an intimate understanding of the behaviors, mindsets, and culture of men in this generation, which I’m able to combine with my scientific background (a dual degree in Biology & Exercise Science) to formulate my own theories as to why testosterone levels are declining in AYA men.
Low Testosterone: Causes & Solutions
In order to identify the causes of testosterone decline, the researchers adjusted their data to account for several factors that are known to affect testosterone levels.
They found that, even after accounting for aging, body mass index (BMI), comorbidity status, alcohol use, smoking status, and physical activity level, the rate of testosterone decline remained statistically significant (12).
Simply put, the usual suspects of low testosterone: getting older, getting fatter, having other health conditions, drinking, smoking, and lack of physical activity did not entirely cause the 25% decline, meaning there were other unknown contributing factors.
This begs the question: what else caused these declines?
At the end of the study, the researchers discussed their hypotheses. Here's what they concluded.
Cause: Phytoestrogens

The researchers postulated that a greater intake of phytoestrogens (compounds from certain plant-based foods that have a structure similar to estrogen) could be a contributing factor (12).
However, given that a more recent and comprehensive meta-analysis found that phytoestrogens do not affect testosterone levels (17), phytoestrogen intake is unlikely to be a notable cause of testosterone decline.
Cause: Poor Body Composition & Diet

The researchers also hypothesized that "changes in diet may alter body composition and body fat percentage independent of BMI, leading to changes in TT levels." (12)
Translation: Even if a man's weight is considered "normal,” if he has a low muscle to fat ratio, his testosterone levels will suffer.
Simply put; being "skinny-fat" lowers testosterone levels, and a low-quality diet is a significant cause.
I wholeheartedly agree with this point. BMI is an inadequate health indicator because it fails to consider body fat percentage and muscle mass, both of which are heavily influenced by diet quality.
Poor Body Composition Solution Pt.1: Lose Body Fat

The optimal body fat percentage for healthy testosterone production ranges between about 10-20% for most men.
If your body fat percentage is significantly above this range, losing body fat is the single most important step you can take to improve your testosterone levels.
This is because adipose tissue (body fat) contains an enzyme called aromatase, which converts testosterone into estrogen.
Common Fat Loss Mistake
A common mistake men make (one I’ve seen several times working with clients) is losing weight too fast, which can lower testosterone levels (1), leading to muscle loss and metabolic slowdown; both of which make continued fat loss extremely challenging.
Generic fat loss advice will recommend reducing calories or losing weight by a fixed amount (ex. “lose 1 pound per week,” or “eat in a 500 calorie deficit”). The problem with these blanket guidelines is they fail to account for the relative size of each individual.
Think about it. A 150 pound man losing 1 pound per week is losing 0.67% of his body weight, whereas a 300 pound man losing 1 pound per week is losing 0.33% of his body weight.
Generic fat loss guidelines also fail to account for one’s current body fat percentage. Fat loss rates should align with initial body fat percentage: faster for higher percentages, slower for lower.
Losing fat as a percentage of your body weight solves both problems: you lose fat at a rate that is proportional to your unique body mass and body fat percentage.
Optimal Fat Loss Guidelines
Aim to lose 0.5-1.5% of your body weight per week based to your current body fat percent:
0.5% per week for leaner individuals (10–15% body fat)
1% per week is a solid middle ground (15–25% body fat).
1.5% per week is reasonable for those carrying higher body fat (25%+).
The beauty of this approach is your weight loss will naturally taper off as you get lighter, which is crucial for preventing reductions in testosterone and weight loss relapses that occur from excessively rapid weight loss.
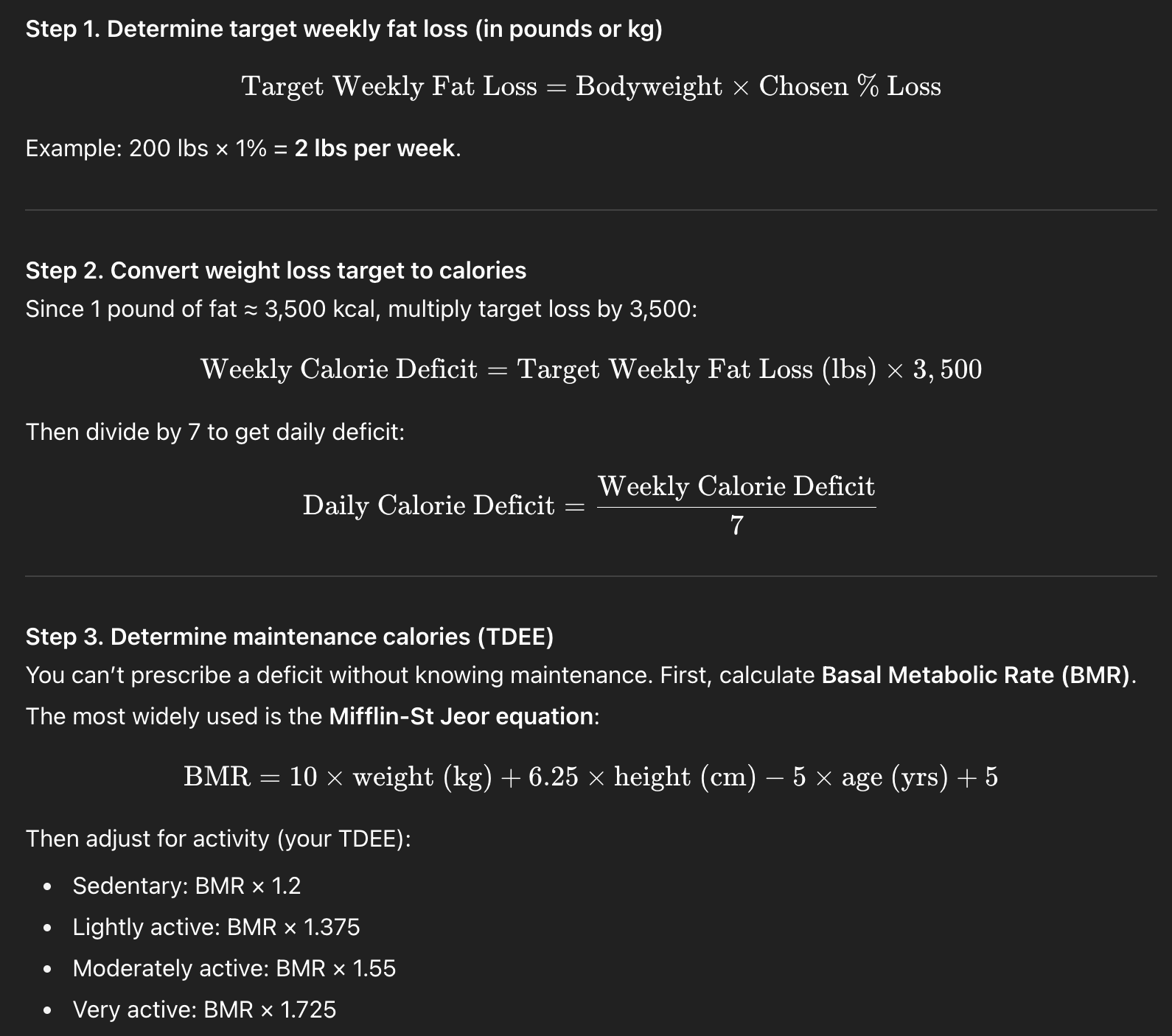
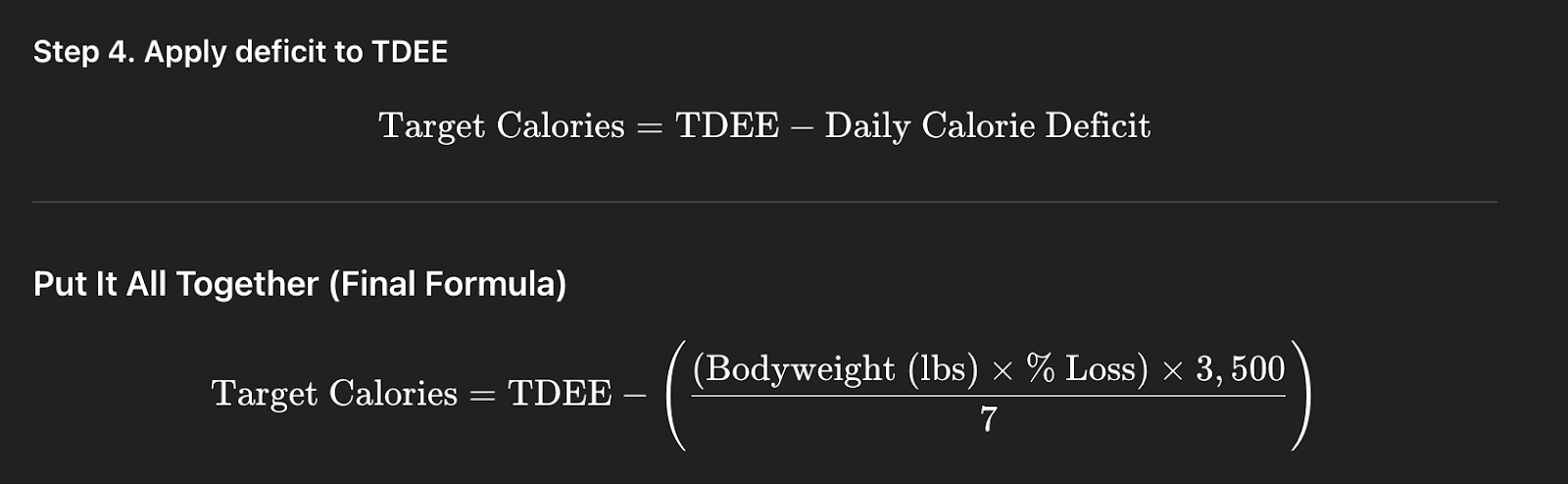
Here’s the formula for how to calculate the calorie deficit you should be in to lose 1% of your body weight per week.
Step 3. Use this TDEE calculator to estimate your Total Daily Energy Expenditure (the number of calories you burn in a day).
Example (200 lb, 5’10”, 30 years old, moderately active, aiming for 1%/week):
- Step 1: Target loss = 200 × 0.01 = 2 lbs/week
- Step 2: Weekly deficit = 2 × 3,500 = 7,000 kcal → 1,000 kcal/day
- Step 3: TDEE ≈ 2,914 kcal
- Step 4: Target intake = 2,914 – 1,000 = 1,914 kcal/day
Poor Body Composition Solution Pt.2: Build Muscle

While losing excess body fat is the single most powerful measure you can take to improve your testosterone levels, as we’ve established, a lack of muscle mass is another contributor to low testosterone, so you also need to build a foundation of muscle.
How to build muscle:
- Lift weights 3-5x per week, prioritizing compound exercises that use multiple muscle groups at the same time, like squats, deadlifts, overhead press, and chin ups.
- Aim for 10-20 sets per muscle group per week.
- Progressively overload by steadily increasing the weight, reps, or sets each week.
- Eat 1g of protein per pound of bodyweight.
Building muscle has a dual benefit for improving your testosterone profile because the very act of lifting weights, if executed consistently, will increase your testosterone levels independent of increased muscle mass.
That said, your weight lifting efforts will be in vain without proper nutrition, so you’ll also need to…
Solution: Improve Your Diet Quality

As mentioned before, the researchers stated that changes in diet may alter body composition leading to lower testosterone levels, but they didn’t define what is meant by “changes in diet.”
Since this study reported that the consumption of processed foods has steadily increased between 2001-2018 (8), I’m going to define “changes in diet” as increased consumption of processed foods.
Here we see another inverse correlation: as consumption of processed foods has increased, testosterone levels have decreased.

This inverse correlation is supported by evidence of causation. A 2023 review established that consumption of ultra processed foods is negatively associated with markers of male reproductive health (21).
Processed foods are broadly defined as “foods that have undergone some form of alteration from their natural state,” and they include just about any food that comes to mind when you think of “junk food.”
Here are some common categories of processed foods:
- Fast food and fried foods: Burgers, fries, fried chicken, pizza — calorie-dense, low in nutrients, often cooked in inflammatory seed oils.
- Packaged snacks: Chips, cookies, crackers, granola bars, trail mixes with added sugars/oils.
- Ready-made meals: Frozen dinners, microwaveable entrees, instant noodles.
- Sugar-sweetened beverages: Sodas, energy drinks, flavored juices, sweet teas.
- Processed meats: Bacon, sausage, hot dogs, deli meats — high in sodium, nitrates, and preservatives.
- Refined grain products: White bread, pastries, sweetened cereals, pasta made from refined flour.
- Ultra-processed dairy substitutes: Flavored yogurts, ice creams, pudding cups.

Due to their hyperplatability and high caloric density, consumption of processed foods is associated with weight gain (3), which we’ve established is the primary risk factor for low testosterone.
Additionally, almost all processed foods also contain a number of artificial additives that are harmful to human health, including:
- Refined sugars: Table sugar, high-fructose corn syrup (HFCS).
- Seed oils: Soybean, canola, corn, sunflower, cottonseed oils — pro-inflammatory when consumed in excess.
- Artificial sweeteners: Aspartame, sucralose, acesulfame-K — can disrupt gut microbiota and appetite regulation in some individuals.
- Trans fats: Partially hydrogenated oils (banned in many countries but still found in some processed imports).
- Preservatives: Sodium nitrite/nitrate, BHA, BHT, sodium benzoate.
- Dyes and colorings: Red 40, Yellow 5, Blue 1 — linked to hyperactivity and inflammation.
- Flavor enhancers: Monosodium glutamate (MSG), “natural flavors” (which are often chemically engineered).
- Emulsifiers and stabilizers: Polysorbate 80, carrageenan, carboxymethylcellulose — associated with gut inflammation and microbiome disruption.
What's more, processed foods have minimal nutritional value; they tend to lack the vitamins and minerals our bodies need for ideal health and testosterone production.
In summary, these are the three outstanding problems with processed food:
- They lead to weight gain because they are easily consumed and calorically dense.
- They contain artificial additives that actively undermine human health.
- They lack beneficial nutrients that contribute to human health.
For these reasons, removing processed foods from one’s diet is a wise decision.
After seeing the food choices made by AYA men in dining halls and dorms, as well as the initial food logs made by new clients, I can say from experience that most AYA men consume far too much processed food.
Based on the data and what I’ve personally witnessed, I’m of the conviction that increased processed food consumption is one of the leading causes of testosterone decline.
The Best Diet For Testosterone Optimization
To protect yourself from the perils of processed foods, I highly recommend following the paleo diet; the very diet I followed on my journey to overcome low testosterone.
The paleo diet emulates the eating patterns of our Paleolithic ancestors, which involves eating nothing but fresh meats, seafood, eggs, fruits, vegetables, nuts & seeds.
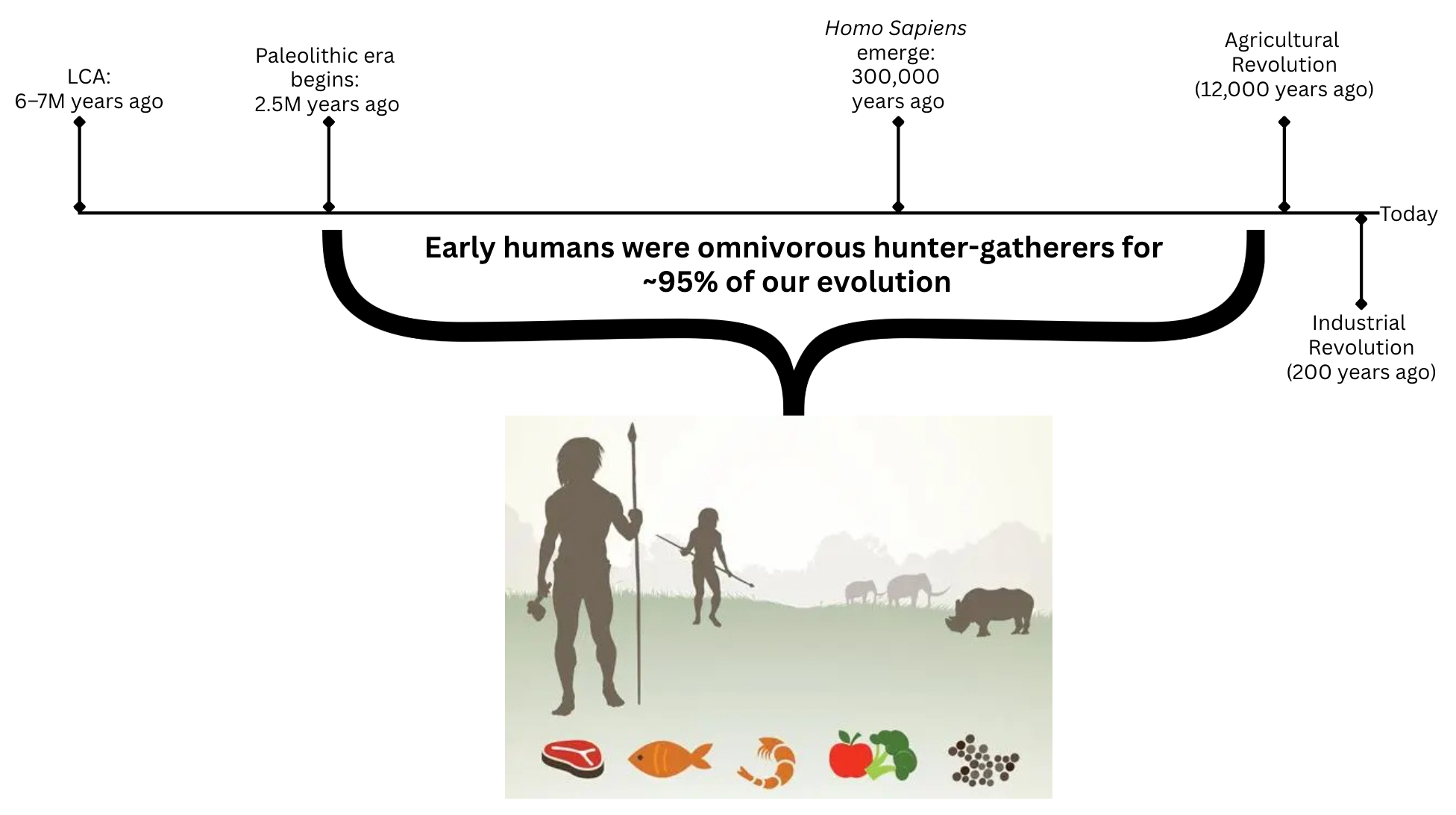
What makes the paleo diet unique is that it is the only diet that explicitly excludes processed foods, because our Paleolithic ancestors would not have had access to them.
Since the paleo diet consists of a wide variety of fruits, vegetables and fresh meats, it also delivers all of the vitamins and minerals your body needs to optimize testosterone production.

If you'd like to learn more about the benefits of the paleo diet and how to follow it, I have another post entirely dedicated to it here.
To make the paleo diet as simple as possible, ask yourself "would a caveman have had access to this food?" If the answer is no, it's not something humans should be eating, and is not optimal for testosterone production.
Cause: Environmental Toxins
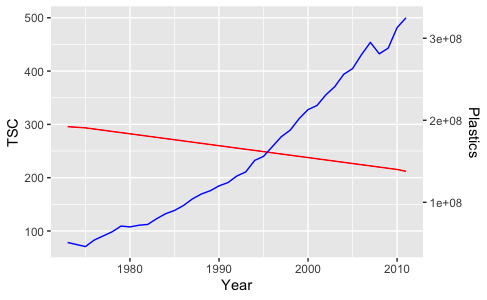
The researchers went on to mention that higher levels of exposure to environmental toxins called endocrine disrupting chemicals (EDCs) may also be driving reductions in testosterone levels (12).
EDCs are chemicals that get into our bodies and disrupt hormone production, leading to a number of negative consequences, including lower testosterone levels and sperm counts (5).
My take: This is one of the most underreported contributors to testosterone decline.
I spent my entire senior year of undergrad researching correlations between the prevalence of EDCs and markers of male reproductive health (sperm counts & testosterone levels), and discovered a statistically significant inverse correlation between them.
To learn more about the how EDCs disrupt male reproductive health, you can read the entire thesis here.
Solution: Avoid Endocrine Disruptors
The two primary sources of EDCs are plastics and pesticides. To avoid them:
- Limit eating and drinking out of plastic containers (Tupperware, water bottles, plastic utensils, etc).
- Buy organic fruits and vegetables & always wash with baking soda before eating.
- Invest in a reverse osmosis filter for your drinking water.
- Only use personal care products that specify "phthalate free."
- Vote for legislation to reduce the usage of plastic and pesticides.
Entire books have been written on the sources of these chemicals, so if you'd like more detail on how to avoid them, you can check out my EDC removal guide.
Cause: Marijuana

The last potential cause of testosterone decline the researchers postulated was increased marijuana use (12), which has been associated with lower testosterone levels in some studies (14), although results are mixed.
Stronger research shows that marijuana use reduces sperm quality (14), to such an extent that fertility clinics advise conceiving couples to stop using it while trying to conceive .
Solution: Avoid Marijuana
Since the male reproductive system is interconnected, and marijuana use is shown to lower sperm quality, it's likely that its effects on testosterone production are negative.
Generally speaking, cutting out anything that is deleterious to your overall health will improve your testosterone production, including substances like marijuana, alcohol, and vapes.
Other Causes Of Low Testosterone
The causes above were all hypothesized to contribute to testosterone decline by the researchers, but based on my experience, there's a few more possible contenders that are worth mentioning.
After spending years researching testosterone, one of the most important things I’ve learned is that the mind has an equally powerful effect on testosterone production as the body.
These effects are called neuro-endocrine interactions (“neuro” = brain) (“endocrine” = hormones), and their influence on societal trends in testosterone levels are presently overlooked.
Men's Mental Health

Depression
There is a bidirectional relationship between depression and low testosterone: low testosterone can give rise to depression, and depression can cause low testosterone (4).
I’ve seen this firsthand with one of my clients. He came to me with numerous signs of low testosterone, one of which was major depression.
After working with him to optimize his testosterone levels naturally, he was able to stop using SSRIs and has reported significantly improved mental health.
Chronic Stress
The stress hormone cortisol competitively inhibits testosterone’s functions; it blocks testosterone from exerting its effects.
Given that rates of both depression and stress have consistently risen in men over 21st century (17), and both are tied to low testosterone, poor mental health seems to be yet another contributor to testosterone decline.
If you struggle with mental health as a man, I highly recommend meditation, stoicism, and journaling. This trifecta has done wonders for my mental health and that of my clients. Another option for you is cognitive behavioral therapy, for which there are many affordable online options.
Lack of Camaraderie
Since the dawn of humankind, men have always had companionship with other men. Cavemen hunted down wooly mammoths together, so this social need for “brotherhood” is encrypted in our genes.

Sadly, a recent survey found that 15% of men today say they have no close friendships, a fivefold increase since 1990.
Based on my 10 years as a football player, I can report that few experiences are as enlivening as being a member of a tribe of men working toward a common goal.

The disappearance of male social bonding is certainly worth considering in the conversation about testosterone decline.
If you lack camaraderie with other men, martial arts studios, recreational sports, and group fitness classes are all great places to start your search for an uplifting community of high quality men to connect with.
Pornography
A 2021 study reported that internet pornography use increased 310% between 2004-2016, that internet pornography viewership was almost twice as common among males than females, and that pornography use was most popular in the 18-27 age group (11).
Surveys conducted by addictionhelp.com found 57% of young adults (18-34) use porn monthly or more often.
Interestingly, pornography use has increased at the same time that testosterone levels have decreased.

There is plausible causation to support this correlation.
A small but interesting study found that testosterone levels peaked at 145.7% above baseline after one week of abstinence from ejaculation (confirm) (6).
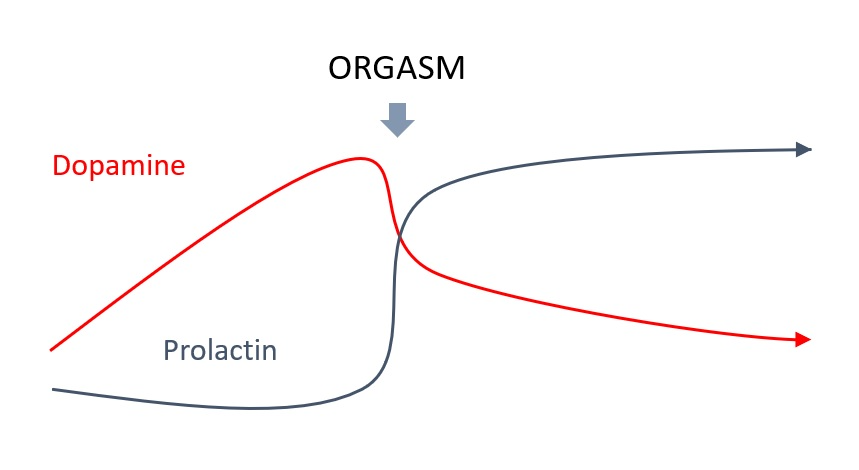
The effect of ejaculation on testosterone is likely related to interactions with the hormone prolactin. Prolactin has the inverse functions as testosterone and temporarily spikes following ejaculation.
It’s also been shown that a daily ejaculation is negatively associated with semen volume, total motile count (TMC) and sperm concentration (20).
Since the male reproductive system is intimately connected, it's plausible that excessive ejaculation could reduce testosterone levels, the same way it can lower semen quality.
Therefore, it follows that if the use of internet pornography has dramatically risen, men are likely ejaculating more frequently at the societal level, possibly contributing to testosterone decline.
Impact of Testosterone Decline on Society
As you can see, testosterone decline is a complex and all-encompassing issue, with reverberating effects on all aspects of a man’s life that extend beyond the individual into society at large.
Testosterone drives motivation, status seeking, and leadership (22), so an entire generation of men with declining testosterone levels could lead to a less productive society overall.
Declines in testosterone have been paralleled by declines in sperm count (10), which makes sense because testosterone drives sperm production.
Since a functional male reproductive system is required for human fecundity, if measures aren’t taken to counteract male reproductive decline, we may see a future in which natural conception is an artifact of the past, and Assisted Reproductive Technologies, which currently have concern worthy effects for mothers and offspring (2), are the norm for human reproduction.
For more on this topic, I highly recommend reading Count Down, by Shanna Swan & Stacey Colino).
Conclusion
I hope that this article has inspired you to take measures not only to protect your own reproductive health, but also to spread your newfound awareness of these issues to others.
If you know of anyone who could benefit from the information presented here, feel free to share this article with them.
If there’s anything you should take away from this article, it's this: the most important thing you can do to optimize your testosterone levels is to become as healthy as possible; mentally, physically, socially, spiritually, and sexually, because above all else, a man's testosterone levels are a reflection of his holistic wellbeing.
That's exactly what I help men do in the Testosterone Transformation Academy; a one-on-one men’s health coaching program I’ve developed to help men optimize their testosterone levels naturally. If that sounds like something you could benefit from, follow the link below for more information.

Optimize Your Testosterone Levels Naturally in the Testosterone Transformation Academy
For more articles like this one, subscribe below.
If you'd like to learn about this subject in video format, check out this video on my Youtube Channel.
References
- Cangemi, R., Friedmann, A. J., Holloszy, J. O., & Fontana, L. (2010). Long-term effects of calorie restriction on serum sex-hormone concentrations in men. Aging Cell, 9(2), 236–242. https://doi.org/10.1111/j.1474-9726.2010.00553.x
- Graham, M. E., Jelin, A., Hoon, A. H., Jr, Wilms Floet, A. M., Levey, E., & Graham, E. M. (2023). Assisted reproductive technology: Short- and long-term outcomes. Developmental Medicine and Child Neurology, 65(1), 38–49. https://doi.org/10.1111/dmcn.15332
- Hall, K. D., Ayuketah, A., Brychta, R., Cai, H., Cassimatis, T., Chen, K. Y., Chung, S. T., Costa, E., Courville, A., Darcey, V., Fletcher, L. A., Forde, C. G., Gharib, A. M., Guo, J., Howard, R., Joseph, P. V., McGehee, S., Ouwerkerk, R., Raisinger, K., Rozga, I., … Zhou, M. (2019). Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell metabolism, 30(1), 67–77.e3. https://doi.org/10.1016/j.cmet.2019.05.008
- Indirli, R., Lanzi, V., Arosio, M., Mantovani, G., & Ferrante, E. (2023). The association of hypogonadism with depression and its treatments. Frontiers in Endocrinology, 14, 1198437. https://doi.org/10.3389/fendo.2023.1198437
- Jeng, H. A. (2014). Exposure to endocrine disrupting chemicals and male reproductive health. Frontiers in Public Health, 2, 55. https://doi.org/10.3389/fpubh.2014.00055
- Jiang, M., Xin, J., Zou, Q., & Shen, J. W. (2003). A research on the relationship between ejaculation and serum testosterone level in men. Journal of Zhejiang University. Science, 4(2), 236–240. https://doi.org/10.1631/jzus.2003.0236 (Retraction published J. Zhejiang Univ. Sci. A. 2021. https://doi.org/10.1631/jzus.2003.r236)
- Jordan, T., Ngo, B., & Jones, C. A. (2020). The use of cannabis and perceptions of its effect on fertility among infertility patients. Human Reproduction Open, 2020(1), hoz041. https://doi.org/10.1093/hropen/hoz041
- Juul, F., Parekh, N., Martinez-Steele, E., Monteiro, C. A., & Chang, V. W. (2022). Ultra-processed food consumption among US adults from 2001 to 2018. The American Journal of Clinical Nutrition, 115(1), 211–221. https://doi.org/10.1093/ajcn/nqab305
- Ko, E. Y., Siddiqi, K., Brannigan, R. E., & Sabanegh, E. S., Jr. (2012). Empirical medical therapy for idiopathic male infertility: A survey of the American Urological Association. The Journal of Urology, 187(3), 973–978. https://doi.org/10.1016/j.juro.2011.10.137
- Levine, H., Jørgensen, N., Martino-Andrade, A., Mendiola, J., Weksler-Derri, D., Jolles, M., Pinotti, R., & Swan, S. H. (2023). Temporal trends in sperm count: a systematic review and meta-regression analysis of samples collected globally in the 20th and 21st centuries. Human reproduction update, 29(2), 157–176. https://doi.org/10.1093/humupd/dmac035
- Lewczuk, K., Wójcik, A., & Gola, M. (2022). Increase in the prevalence of online pornography use: Objective data analysis from the period between 2004 and 2016 in Poland. Archives of Sexual Behavior, 51(2), 1157–1171. https://doi.org/10.1007/s10508-021-02090-w
- Lokeshwar, S. D., Patel, P., Fantus, R. J., Halpern, J., Chang, C., Kargi, A. Y., & Ramasamy, R. (2021). Decline in serum testosterone levels among adolescent and young adult men in the USA. European Urology Focus, 7(4), 886–889. https://doi.org/10.1016/j.euf.2020.02.006
- Okobi, O. E., Khoury, P., De la Vega, R. J., Figueroa, R. S., Desai, D., Mangiliman, B. D. A., Vera Colon, O. L., Urruela-Barrios, R. J., Abdussalam, A. K., Diaz-Miret, M., & Hernandez Borges, S. (2024). Impact of weight loss on testosterone levels: A review of BMI and testosterone. Cureus, 16(12), e76139. https://doi.org/10.7759/cureus.76139
- Patel, A. S., Leong, J. Y., Ramos, L., & Ramasamy, R. (2019). Testosterone is a contraceptive and should not be used in men who desire fertility. The World Journal of Men's Health, 37(1), 45–54. https://doi.org/10.5534/wjmh.180036
- Payne, K. S., Mazur, D. J., Hotaling, J. M., & Pastuszak, A. W. (2019). Cannabis and male fertility: A systematic review. The Journal of Urology, 202(4), 674–681. https://doi.org/10.1097/JU.0000000000000248
- Rao, P. K., Boulet, S. L., Mehta, A., Hotaling, J., Eisenberg, M. L., Honig, S. C., Warner, L., Kissin, D. M., Nangia, A. K., & Ross, L. S. (2017). Trends in Testosterone Replacement Therapy Use from 2003 to 2013 among Reproductive-Age Men in the United States. The Journal of urology, 197(4), 1121–1126. https://doi.org/10.1016/j.juro.2016.10.063
- Reed, K. E., Camargo, J., Hamilton-Reeves, J., Kurzer, M., & Messina, M. (2021). Neither soy nor isoflavone intake affects male reproductive hormones: An expanded and updated meta-analysis of clinical studies. Reproductive Toxicology, 100, 60–67. https://doi.org/10.1016/j.reprotox.2020.12.019
- Suicide mortality in the United States, 2002–2022. (2023, November 28). Centers for Disease Control and Prevention. https://www.cdc.gov/nchs/products/databriefs/db509.htm
- Travison, T. G., Araujo, A. B., O'Donnell, A. B., Kupelian, V., & McKinlay, J. B. (2007). A population-level decline in serum testosterone levels in American men. The Journal of Clinical Endocrinology and Metabolism, 92(1), 196–202. https://doi.org/10.1210/jc.2006-1375
- Welliver, C., Benson, A. D., Frederick, L., Leader, B., Tirado, E., Feustel, P., Kontio, J., McAsey, M., & Köhler, T. S. (2016). Analysis of semen parameters during 2 weeks of daily ejaculation: A first in humans study. Translational Andrology and Urology, 5(5), 749–755. https://doi.org/10.21037/tau.2016.08.20
- Welliver, J. (2023). Dietary trends and the decline in male reproductive health. Hormones (Athens, Greece), 22(2), 165–197. https://doi.org/10.1007/s42000-023-00431-z
- Zitzmann, M. (2020). Testosterone, mood, behaviour and quality of life. Andrology, 8(6), 1598–1605. https://doi.org/10.1111/andr.12867


